Symposium: Ensuring abortion safety in a declining market for abortion services
on Jan 7, 2016 at 9:43 am
Teresa Stanton Collett is Professor at University of St. Thomas School of Law. The views she expresses are hers alone.
Whole Woman’s Health v. Cole involves two contested provisions of a Texas law, referred to as HB2. The first requires abortion practitioners to have admitting privileges at a hospital within thirty miles of where they perform abortions, and the second requires abortion facilities to meet ambulatory-surgical-center (“ASC”) standards governing operating protocols, physical plant, and general safety.
The state argues the admitting-privileges requirement ensures ease of transfer and continuity of care for women needing hospitalization due to injuries or unanticipated conditions arising from their abortions. The ASC requirement is designed to make certain that abortion clinics meet the general safety standards applied to other facilities that operate primarily to provide surgical services (such as cataract removal, colonoscopies, knee arthroscopies, and tonsillectomies).
Abortion providers have attacked these provisions as offering little medical benefit to women, while reducing access to abortion. Ironically the main thrust of their argument is that the Constitution requires both that Texas allow abortion clinics to operate at a lower standard of care than other facilities at which surgeries are routinely performed and that abortion doctors be exempt from the requirement of admitting privileges to nearby hospitals. This bizarre combination of objections leads to the very real possibility that when an injury or complication occurs during or after an abortion, the clinic will be less equipped than an ambulatory surgical center to address the problem on site and more likely to transfer care to an emergency room where the abortion practitioner has no relationship with any of the medical staff. In short, their arguments make it appear that abortion activists care more about access to abortion (safe or unsafe) than they do about protecting women’s health.
Impetus of the legislation
The Texas legislature was prompted to pass HB2 in part by concerns arising from the case of Dr. Kermit Gosnell, the infamous Philadelphia abortionist convicted of three murders and involuntary manslaughter arising from his practice. The Pennsylvania Grand Jury Report describes the scene investigators found when they entered Gosnell’s abortion clinic:
There was blood on the floor. A stench of urine filled the air. A flea-infested cat was wandering through the facility, and there were cat feces on the stairs. Semi-conscious women scheduled for abortions were moaning in the waiting room or the recovery room, where they sat on dirty recliners covered with blood-stained blankets.
. . . .
Investigators found the clinic grossly unsuitable as a surgical facility. The two surgical procedure rooms were filthy and unsanitary – Agent [Stephen] Dougherty described them as resembling “a bad gas station restroom.” Instruments were not sterile. Equipment was rusty and outdated. Oxygen equipment was covered with dust, and had not been inspected. The same corroded suction tubing used for abortions was the only tubing available for oral airways if assistance for breathing was needed. There was no functioning resuscitation or even monitoring equipment, except for a single blood pressure cuff in the recovery room.
At the conclusion of the report, the Philadelphia district attorney’s office made a set of recommendations, including that abortion clinics be regulated as ambulatory surgical centers. Recommendation 5 on page 247 of the report concluded that “[t]here is no justification for denying abortion patients the protections available to every other patient of an ambulatory surgical facility, and no reason to exempt abortion clinics from meeting these standards.”
Trend toward abortions in ASCs
The legislators in Texas (and several other states) agreed with this recommendation and passed HB2 in 2013. This was long after an increasing number of abortions were being performed at Texas clinics classified as ASCs. Annual reports from the Texas Department of Health show that the trend of abortions being performed in ASCs began in 2005 and by 2013, the last year for which statistics are available, almost one-quarter of all abortions in the state were performed at ASCs.
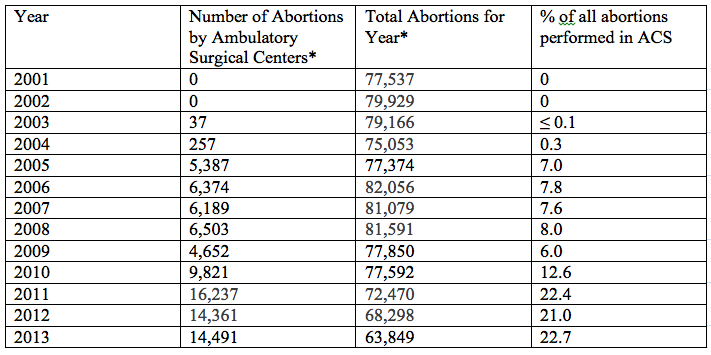
*Numbers are drawn from the Texas Department of State Health Services, Vital Statistics Annual Reports for years 2001-20013, Table 37.
This historical snapshot undercuts any argument that requiring abortion clinics to comply with ASC standards is unrelated to promoting women’s health.
Admitting privileges and the need of coordinated responses
Similarly, historical experience supports the state’s concern regarding effective and coordinated response between abortion providers and hospital personnel when injuries occur during an abortion. For example, Dr. Leroy Carhart, often identified as a hero of the pro-abortion movement, has been investigated repeatedly for dangerous and unprofessional practices. Most recently he was investigated for the death of his patient, Lisa Morbelli. According to a complaint filed with the Maryland Board of Physicians, “[a]fter Morbelli’s abortion, while still appearing ‘weak and pale’ according to witnesses, Carhart released her to return to her hotel. He then left town. As Morbelli’s condition worsened, in the ensuing hours, Carhart could not be reached by family members or later by hospital emergency room staff.” While the board imposed no discipline, the case illustrates the danger to patients when abortion providers are not integrated into the local medical community.
The danger from lack of coordination is even more acute outside major metropolitan areas where specialized emergency care is limited, if available at all. Researchers at the nonpartisan Center for Studying Health System Change have found that “[t]wenty-one percent of patient deaths or permanent injuries related to ED [emergency department] treatment delays are attributed to lack of availability of physician specialists” and “[t]wo-thirds of ED directors in level I and II trauma centers say that more than half of all patient transfers they receive stem from lack of timely access to specialist physicians at the referring hospital.” These issues are of particular concern in a state the size of Texas with broad swathes of rural areas. A 2011 survey of Texas health care revealed that of the 254 counties in Texas, 144 did not have a gynecologist or obstetrician, 138 did not have a pediatrician, and 29 did not have a primary care physician. These access problems are compounded by the fact that there simply is no emergency care to be had in a growing number of counties. Across Texas, ten rural hospitals have closed since 2012, according to data from the National Rural Health Association. The simple fact is that ensuring access to quality health care for people living outside major metropolitan areas is difficult, and Texas is no exception to this rule.
That said, nothing in Supreme Court jurisprudence or common sense requires legislators to exempt abortion from state efforts to ensure the safety of patients undergoing invasive procedures by regulating both the clinics where abortions are performed and the doctors who perform them.
Constitutional challenges ignore economic realities
Abortion activists disregard these facts and instead argue that enforcement of HB2 has and will result in more and more abortion clinics closing, thus unconstitutionally burdening women’s access to abortion. It is clear that abortion clinics are closing in Texas, but exactly why they are closing is hotly disputed.
Some of the decline in the number of abortion clinics can be attributed to the fact that fewer women are seeking abortions. This summer the Associated Press found that there has been a decrease in abortions of about twelve percent since 2010 nationwide. In the same period Texas abortions declined twelve percent. And this decline is part of an even larger decline when the time period is expanded. In Texas there were almost 20,000 fewer abortions reported in 2013 than were reported in 2006. Activists are quick to claim that the decline is due to oppressive state regulations, yet as the AP report noted “[f]ive of the six states with the biggest declines – Hawaii at 30 percent, New Mexico at 24 percent, Nevada and Rhode Island at 22 percent, Connecticut at 21 percent – have passed no recent laws to restrict abortion clinics or providers.” It is simply false to claim that HB2 or any other Texas regulation is the proven cause of falling abortion numbers.
What is true is that abortion clinics are trying to survive in a shrinking market for their services. This is causing an economic restructuring of the abortion industry, in which economies of scale and cost efficiency are increasingly important.
Planned Parenthood, both nationally and in Texas, is aggressively increasing its market share through the creation of “mega-clinics,” making it difficult if not impossible for independent providers to compete. In 2010 Planned Parenthood opened a new 78,000 square foot facility in Houston. According to a May 20, 2010 article in the Houston Chronicle, the new facility provided “room to increase Texas clients by 30 percent, from 90,000 visits to those 10 locations in 2009 to roughly 120,000 annually.” In 2014 Planned Parenthood in San Antonio opened a new 22,000-square-foot facility. Planned Parenthood Affiliate President Jeffery Hons told the local newspaper that the new center will perform about 2,800 abortions a year — an increase of 1,000 over the number provided two years ago, before HB 2.” That’s an increase of 30,000 visits in Houston plus 1,000 new abortions performed in San Antonio. This sort of increase in capacity makes continued existence of small competitors more difficult regardless of the regulatory environment.
Conclusion
All of these facts – proven cases of unsanitary and dangerous conditions in some abortion clinics; declining numbers of women seeking abortions; restructuring of the abortion industry; shrinking numbers of emergency care providers in rural areas; and greater regulation of health care in general – make the case that the Texas law will improve women’s health care.
The objection of abortion activists to the efforts of Texas can easily be read as demands of a protectionist industry that cares little about the quality of care it delivers and more about its ability to survive in a shrinking market for its services. It would be a height of judicial pretention to constitutionalize these claims into a basis for striking down the Texas law.